
 |
 |
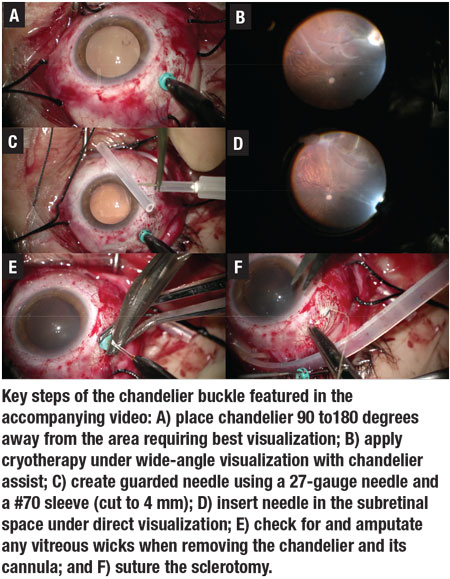
Primary scleral buckle surgery is an important skill for any vitreoretinal surgeon. The use of chandelier illumination during scleral buckle surgery coupled with a microscope-based wide-angle viewing system (“chandelier buckle”) is increasing in popularity. For those interested in exploring this technique or refining their skills, we present six considerations for successful chandelier buckling (Figure).
• Careful preoperative examination. The chandelier should be placed 90 to 180 degrees from the area requiring best visualization (i.e., the site of the retinal breaks that need cryotherapy or the intended location of subretinal fluid drainage). Carefully examine the retinal detachment preoperatively to determine the best location for chandelier placement.
• Trocar placement and management. Insert the chandelier after isolating the rectus muscles and prior to cryotherapy. If possible, use a valved cannula to minimize the risk of vitreous prolapse. Place the trocar with a straight or minimally beveled insertion, which directs illumination toward the center of the vitreous cavity. Or, if you prefer a beveled approach, direct the chandelier toward the area of pathology.
During manipulation of the globe, ensure that the cannula doesn’t become dislodged by the silk sutures or the lid speculum. When removing the chandelier or its cannula, diligently check for and amputate any vitreous wicks. Have a low threshold to suture the sclerotomy. Some surgeons prefer to remove the cannula prior to tightening the buckle to minimize the risk of vitreous prolapse when the intraocular pressure is elevated. Consider applying a few spots of cryotherapy to the area immediately posterior or adjacent to the chandelier site with concern for undue vitreous traction.
• Getting a peripheral view. As with vitrectomy, a peripheral view is obtained by rotating the eye and moving the microscope in the direction of the area of interest. In chandelier buckling, four techniques can be used for moving the eye:
- manipulate one or two of the silk sutures;
- hold the chandelier and use it to maneuver the eye;
- use the cryoprobe or scleral depressor; or,
- most commonly, combine of these techniques.
 |
• Ergonomics. If desired, the entire chandelier buckle procedure, start to finish, can be performed using the microscope without having to rotate the microscope or your position. To accomplish this, I prefer to suture the scleral quadrants on my left with the right hand and those on my right with the left hand.
• Drainage. Subretinal fluid may be drained under direct chandelier visualization. One method (Video) is to introduce a small-gauge needle into the subretinal space through an area of the sclera that’s intended to be supported by the scleral buckle (i.e., within the “bed” of the buckle). For added safety, the needle can be guarded using a silicone sleeve. Using the chandelier, the needle can then be seen within the subretinal space.
• Endolaser probes. Some surgeons have utilized illuminated endolaser probes during chandelier buckling. These can be considered in certain instances, though they may increase the risk of vitreous traction and iatrogenic breaks. RS
Watch as Dr. Ali performs a scleral buckling procedure with chandelier illumination.



