ABOUT THE AUTHOR | |
 | Dr. Jumper is in private practice with West Coast Retina in San Francisco, CA. He is co-director of the vitreoretinal fellowship program at California Pacific Medical Center. |
Risk Factors
The main risk factors for RVO include age and systemic vascular disorders. A study in Israel found that the rate of RVO increased exponentially with age—from 0.93 per 1,000 in people age 64 years and younger to 5.36 per 1,000 for those 65 and older.2 That said, RVO can occur at any age. Sohan Singh Hayreh, MD, PhD, DSc, and colleagues study reported that 49 percent of RVO patients were younger than 65 years old. Also, a significant percentage were younger than 45; 15 percent for central RVO (CRVO), 10 percent for hemi-CRVO and 5 percent for BRVO.3Hypertension, hyperlipidemia and diabetes, all atherosclerotic risk factors, are strongly associated with RVO development. Paul R.A. O’Mahoney, MD, and co-authors calculated the population-attributable risk percentage of these factors and found that 46 percent of RVO cases are due to hypertension, 20 percent due to hyperlipidemia and 5 percent due to diabetes.4 This emphasizes that, while RVO is indeed an occlusion of a retinal venule, the condition is primarily a consequence of atherosclerosis of the adjacent arteriole.
History and Examination
With this in mind, a systemic evaluation of RVO should include a thorough medical history that investigates atherosclerotic risk factors such as hypertension, hyperlipidemia, diabetes, smoking, obesity and family history of coronary artery disease. An assessment for hypercoagulability risk factors should also take into account estrogen exposure, malignancy, pregnancy or a family history of thrombophilia before age 50 years.Glaucoma and ocular hypertension are risk factors for CRVO. This underscores the importance of inquiring about a family history of glaucoma and evaluating both eyes for glaucoma, keeping in mind that intraocular pressure (IOP) may be lower in an eye with acute CRVO.5
Blood pressure should be measured not only in the office but also serially to rule out masked hypertension. Many patients with elevated blood pressure measured in the office will manifest “white-coat hypertension,” which carries a strong risk of conversion to sustained hypertension over time.6
 |
 |
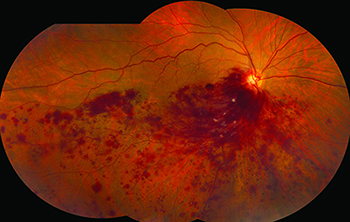
In the acute phase, hemorrhage can create blockage of fluorescence, making it difficult to evaluate vascular perfusion. In RVO with severe hemorrhage, one should consider obtaining color fundus images and deferring angiography until the blood clears and more information can be obtained (Figure 1). If a patient with RVO has a fluorescein angiogram, late images of the iris of both eyes can help identify rubeosis.
With advances in imaging technology, the benefits of widefield fluorescein angiography have been shown in detecting peripheral ischemia not otherwise visible.8 Spectral domain or swept-source optical coherence tomography (OCT) is also important in assessing macular edema in RVO and should be done initially and to follow therapy response.
Controversy of Lab Testing
The most controversial issue in the RVO workup involves the utility of laboratory testing. A reasonable approach is to consider a directed assessment of atherosclerotic risk factors for any patient with an RVO. These include a lipid profile, blood glucose measurement and complete blood count. Atypical features such as intraocular inflammation should lead to further testing for conditions such as sarcoidosis, syphilis and systemic lupus erythematosus.Over the past two decades, a number of mostly small series and case reports have explored the role of thrombophilic abnormalities in RVO development. Inherited thrombophilic defects include deficiencies of antithrombin, protein C and protein S, factor V Leiden and the prothrombin G20210A mutation.
Acquired risk factors for thrombosis include the antiphospholipid antibody syndrome, myeloproliferative disorders, immobilization, major surgery, malignancy, estrogens and heparin-induced thrombocytopenia. Other risk factors include hyperhomocysteinemia and elevated factors VIII, IX and XI. Of all of these abnormalities, only hyperhomocysteinemia and the antiphospholipid antibody syndrome are associated with both arterial and venous thrombosis. All other defects are classical venous thrombophilias (Table, page 23).
A young patient with a RVO and no identifiable risk factors will typically undergo an extensive battery of tests looking for some or all of the thrombophilia risk factors. Research indicates that this approach is rarely helpful. Danish researcher Prof. Janne Ingerslev said, “Most well characterized risk factors for general venous thrombosis occur sporadically in RVO, and have no major importance in the pathophysiology of RVO.”9
Italian investigators found no difference between RVO patients and age/sex matched controls in levels of antithrombin, protein C, protein S and homocysteine, lupus anticoagulant, anticardiolipin antibodies or prothrombin polymorphisms.10 In this same study, arterial hypertension and diabetes were the only factors more common to the RVO patients compared to controls (Figure 2).
Dutch investigators found the two risk factors for arterial thrombosis—hyperhomocysteinemia and the antiphospholipid antibody syndromes—were associated with RVO.11 J. Michael Lahey, MD, and colleagues studied young patients with CRVO and found at least one thrombophilia lab abnormality in 27 percent of subjects, most commonly elevated homocysteine levels and antiphospholipid antibody titers,12 which supports the Dutch study. In Dr. Lahey’s study, the one patient with a systemic disease (protein S deficiency) had bilateral CRVO.
 |
The only other treatment option for a patient with a thrombophilia is long-term anticoagulation. RVO is unlike a deep venous thrombosis where anticoagulation is used to prevent a downstream pulmonary embolism. Little evidence exists that anticoagulation prevents further ocular vascular occlusion. Anticoagulation has no known benefit on the active clot. Also, in the acute phase of an RVO, anticoagulation may be harmful to the neural retinal tissue by increasing intraretinal hemorrhage, as Dr. Hayreh pointed out.14
Conclusion
RVO can happen at any age but is most common in patients over age 65. Vein occlusion shares risk factors of atherosclerosis. The clinician should direct the workup toward evaluation of hypertension, hyperlipidemia and diabetes.Thrombophilia testing is rarely needed, but can be considered in patients who have a family history of clotting under the age of 50, a personal history of clotting or an unusual presentation such as bilateral simultaneous occlusion.
Consider testing for clotting defects associated with arterial disease, including the antiphospholipid antibody syndrome and hyperhomocysteinemia. Even if a clotting abnormality is discovered, it may or may not be related to the ocular condition. Furthermore, treatment in the acute phase, especially with anticoagulation, may do more harm than good. RS
Disclosure: Dr. Jumper has no relevant conflicts to disclose.
References
1. Rogers S, McIntosh RL, Cheung N, et al. The prevalence of retinal vein occlusion: pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology. 2010; 117:313.e1–319.e1.2. David R, Zangwill L, Badarna M, Yassur Y. Epidemiology of retinal vein occlusion and its association with glaucoma and increased intraocular pressure. Ophthalmologica. 1988;197;69–74.
3. Hayreh SS, Zimmerman MB, PodhajskyP. Incidence of various types of retinal vein occlusion and their recurrence and demographic characteristics. Am. J. Ophthalmol. 1994;117:429–441.
4. O’Mahoney PR, Wong DT, Ray JG. Retinal vein occlusion and traditional risk factors for 4therosclerosis. Arch Ophthalmol. 2008;126:692-699.
5. Hayreh SS, March W, Phelps CD. Ocular hypotony following retinal vein occlusion. Arch. Ophthalmol. 1978;96:827–833.
6. Mancia G, Bombelli M, Facchetti R, et al. Long-term risk of sustained hypertension in white-coat or masked hypertension. Hypertension, 2009;54:226-232.
7. Hayreh SS, Klugman MR, Beri M, Kimura AE, Podhajsky P. Differentiation of ischemic from non-ischemic central retinal vein occlusion during the early acute phase. Graefe’s Arch Clin Exp Ophthalmol. 1999;228:201-217.
8. Spaide RF. Peripheral areas of nonperfusion in treated central retinal vein occlusion as imaged by wide-field fluorescein angiography. Retina. 2011;31:829-837.
9. Ingerslev J. Thrombophilia: a feature of importance in retinal vein thrombosis? Acta Ophthalmol Scand. 1999;77:619–621.
10. Di Capua M, Coppola A, Albisinni R, et al. Cardiovascular risk factors and outcome in patients with retinal vein occlusion. J Thromb Thrombolysis. 2010; 30:16-22.
11. Janssen MC, den Heijer M, Cruysberg JR, et al. Retinal vein occlusion: a form of venous thrombosis or a complication of atherosclerosis? A meta-analysis of thrombophilic factors. Thromb Haemost. 2005; 93:1021-1026.
12. Lahey JM, Tunc M, Kearney J, et al. Laboratory evaluation of hypercoagulable states in patients with central retinal vein occlusion who are less than 56 years of age. Ophthalmology. 2002;109:126–131
13. The VITATOPS Trial Study Group. B vitamins in patients with recent transient ischaemic attack or stroke in the VITAmins TO Prevent Stroke (VITATOPS) trial: a randomised, double-blind, parallel, placebo-controlled trial. Lancet Neurol. 2010;9:855–865.
14. Hayreh SS. Prevalent misconceptions about acute retinal vascular occlusive disorders. Prog Retinal Eye Res. 2005;24:493–519.



