
 |
Bios Dr. Hahn is a partner at New Jersey Retina in Teaneck. DISCLOSURES: Dr. Lee reports financial relationships with Allergan/AbbVie, Alimera Sciences, Apellis Pharmaceuticals and EyePoint Pharmaceuticals. Dr. Hahn is a consultant to DORC. |
 |
|
In the video below, Dr. Lee demonstrates his technique for creating subretinal blebs without a retinotomy to repair recalcitrant or chronic full-thickness macular holes. |
Refractory macular holes or failed hole closures are inevitable, although infrequent. I’ve tried various techniques with varying success. Free flaps are difficult to maneuver and keep in place. Brushing the nerve fiber layer with a diamond-dusted scraper seems to induce more damage than it creates elasticity.
I had better outcomes with perifoveal subretinal balanced salt solution injections, particularly in cases with smaller holes (<500 µm) than the chronic large holes that might require retinal transplant or amniotic membrane graft.
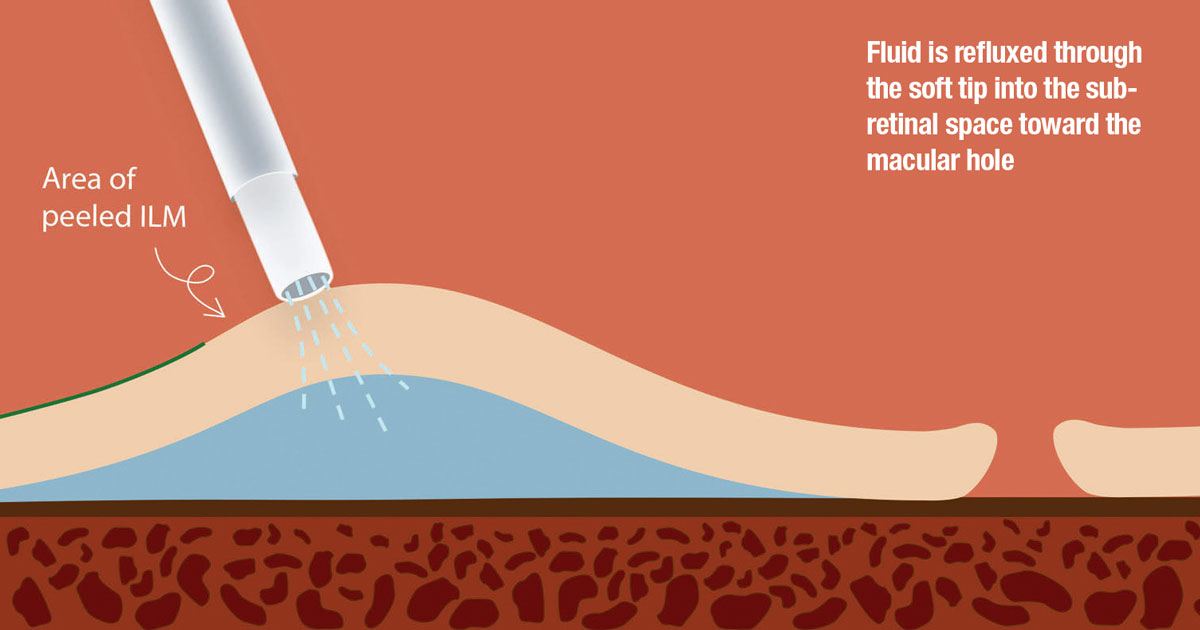
However, I wondered if it was really necessary to pierce the retina with a subretinal cannula. I thought if you could aspirate subretinal perfluoro-n-octane through an area of peeled internal limiting membrane transretinally (i.e., without a retinotomy), it should work in the reverse: to inject BSS transretinally without a retinotomy to create a subretinal bleb.
Promising closure rates have been reported with macular detachment with subretinal fluid injections (80 to 90 percent).1-2 Creating increased elasticity of the perifoveal macula allows for the retinal tissue immediately adjacent the hole to close. This can be combined with scaffold techniques.
Surgical technique
The technique uses a standard vitrectomy set up. The soft tip is connected to the extrusion line, which has been primed with BSS. The amount of fluid in the tubing varies between manufacturers, but it’s typically >10cc.
If not already done, then the ILM must be peeled to facilitate transretinal fluid passage. The extrusion line with the soft tip is then set to proportional reflux (standard settings on Alcon Constellation are 0 to 120 mmHg) and checked to make sure no air, hemorrhage or dye is in the cannula or line.
The soft tip is then placed over the target area, approximately 1 disc diameter from the fovea. The soft tip is positioned to just touch the retinal surface. The fluid is then refluxed with increasing pressure until a bleb of desired size is created (Figure). Generally the amount of pressure needed is 30 to 40 mmHg (25 percent pedal depression). Alternatively, you can set the high end of reflux to 40 mmHg (full pedal depression) to avoid theoretical retinal pigment epithelium trauma from a high-pressure jet stream.
 |
I typically place blebs superotemporally and inferotemporally. I aim to create a bleb that just lifts the edge of the hole rather than refluxing through the hole. This technique can also be performed with a subretinal needle on the extrusion line and requires less pressure since the jet stream of fluid is stronger with a smaller diameter.
For chronic, large holes
This is a helpful adjunctive technique for treating chronic, large holes. My partners at Georgia Retina and I have had good success for >700-µm holes thus far with a 90 percent closure rate and no complications.
In addition to avoiding a retinotomy, this technique uses readily available equipment without the additional cost of a subretinal needle and/or VFC pack. For cases of holes that fail to close after standard initial macular hole surgery, this can be a useful technique as a second surgery prior to plug techniques (e.g., autologous graft or amniotic membrane). RS
REFERENCES
1. Meyer CH, Szurman P, Haritoglou C, et al. Application of subretinal fluid to close refractory full thickness macular holes: Treatment strategies and primary outcome: APOSTEL study. Graefes Arch Clin Exp Ophthalmol. 2020;258:2151–2161.
2. Felfeli T, Mandelcorn ED. Macular hole hydrodissection: surgical technique for the treatment of persistent, chronic, and large macular holes. Retina. 2019;39:743-752.



