
 |
Bios Dr. Hahn is a partner at New Jersey Retina in Teaneck. DISCLOSURES: Dr. Lenis and Dr. Mahrous have no relevant disclosures. Dr. D’Amico is a consultant to Alcon. Dr. Hahn is a conslutant to DORC. |
The creation of a posterior vitreous detachment is critical in pars plana vitrectomy for most macular vitreoretinal interface disorders and retinal detachments. However, PVD induction can be a challenging surgical step in young patients as well as in older patients with particularly adherent posterior hyaloid or abnormal vitreoretinal interface.
Failure to successfully induce PVD can result in poor surgical outcomes such as persistent macular holes and proliferative vitreoretinopathy. Here, we review a variety of surgical methods that can be employed to aid in PVD induction.1
‘Staining’ vitreous
Enhancing visualization of the vitreous with intravitreal agents such as triamcinolone can help you see that the vitreous cutter (or soft-tip) is continuously engaging with the posterior hyaloid on aspiration. This is particularly useful to confirm that the cutter isn’t above the hyaloid face, but, instead, is at an edge or below an edge (in a plane between the hyaloid and retina) allowing you to efficiently aspirate and then lift the hyaloid.
Lack of internal limiting staining with vital dyes such as Brilliant Blue G (DORC) can also often indicate when the posterior hyaloid has not been sufficiently elevated.
Soft-tipped cannula
The use of a soft-tipped cannula can be an efficient alternative to the vitreous cutter, particularly if there’s no obvious opening in the hyaloid face directly below the cutter. Often, if the “edge” can’t be immediately found with the vitreous cutter, it may help to switch to the soft-tip to more directly engage with the posterior hyaloid.2
 |
|
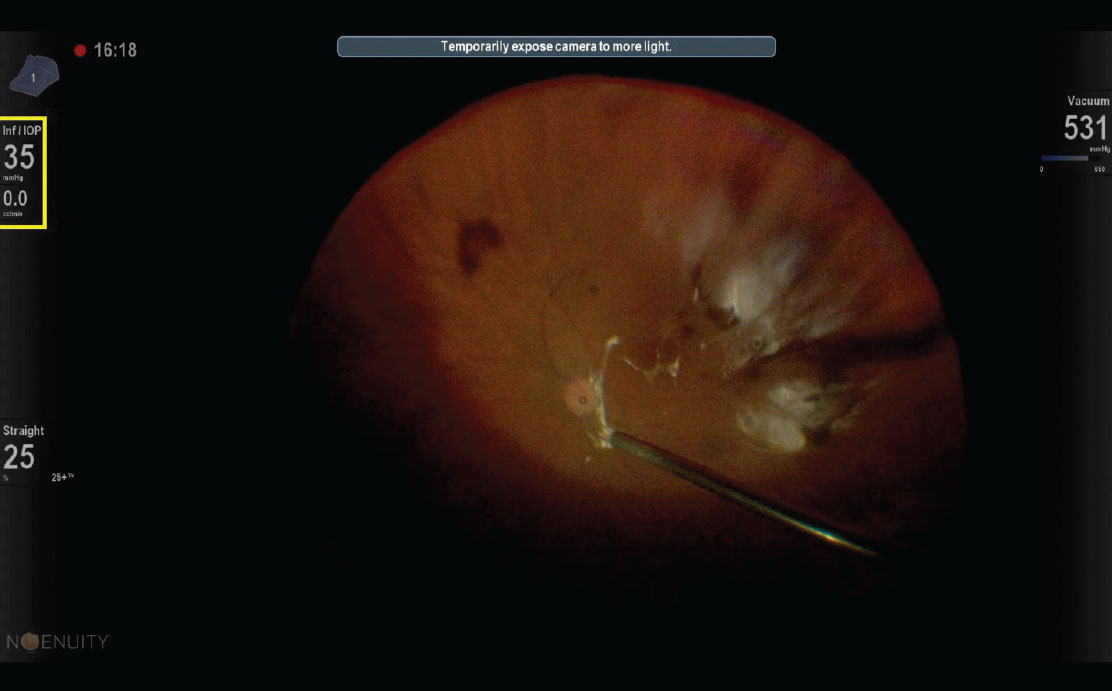
A view of a posterior vitreous detachment using a soft-tipped cannula and the Ngenuity heads-up display (Alcon). Note the upper left inset (yellow box) indicates a flow rate of 0.0 cc/min when the instrument is completely occluded by the posterior hyaloid. |
Sharp dissection of the hyaloid face
If needed, direct sharp dissection of the hyaloid face can also help to create a surgical opening in the posterior hyaloid, if one isn’t already apparent. This technique has been described using a variety of instruments, including the diamond-dusted membrane scraper, micropick, microvitreoretinal blade and barbed needle.3-6
Visual cues on 3D heads-up display indicate occlusion
A built-in aid for PVD induction is to follow flow rates on the vitrectomy machine, taking advantage of the fact that the flow rate, often indicated adjacent to the set infusion pressure, will read near zero when the instrument is effectively occluded by the posterior hyaloid (Figure). This can be ascertained with an assistant giving verbal cues from a conventional display of any of the available vitrectomy platforms.
Alternatively, you can directly view the flow rate on a three-dimensional heads-up display (e.g., Ngenuity, Alcon). In inducing a PVD, when the flow rate drops to zero upon aspiration, simply remain in place while maintaining strong suction with the instrument port occluded for another two to three seconds; then elevation can begin.
A resumption of flow indicates a loss of suction, and the maneuver to reengage the hyaloid can be repeated as necessary. This technique allows you to more precisely and efficiently increase aspiration and lift the posterior hyaloid with confidence. RS
REFERENCES
1. Ellabban AA, Barry R, Sallam AAB. Surgical induction of posterior vitreous detachment using combined sharp dissection and active aspiration. Acta Ophthalmologica. 2016;94:e524-525.
2. Kelly NE, Wendel RT. Vitreous surgery for idiopathic macular holes. Results of a pilot study. Arch Ophthalmol. 1991;109:654–659.
3. Takeuchi M, Takayama K, Sato T, Ishikawa S, Fujii S, Sakurai Y. Non-aspiration technique to induce posterior vitreous detachment in minimum incision vitrectomy system. Br J Ophthalmol. 2012; 96:1378–1379.
4. Han DP, Abrams GW, Aaberg TM. Surgical excision of the attached posterior hyaloid. Arch Ophthalmol. 1988;106:998–1000.
5. Desai UR, Bhatti RA, Khan KA, Rubowitz A. Sharp dissection of the Weiss ring to induce a posterior vitreous detachment. Br J Ophthalmol. 2008;92:420–422.
6. Garg SJ. Use of a suction pick in small-gauge surgery facilitates induction of a posterior vitreous detachment. Retina. 2008;28:1536.



