
 |
| Bios Dr. Read is a partner at Retina Consultants of Hawaii and a clinical assistant professor at University of Hawaii John A. Burns School of Medicine. Dr. Hahn is a partner at New Jersey Retina in Teaneck. Dr. Read disclosed serving as a consultant to Carl Zeiss Meditec. Dr. Hahn disclosed serving as a consultant to DORC. |
Scleral buckling, either as a primary procedure or in combination with vitrectomy, is an important skill for any vitreoretinal surgeon. The six pearls here will help you place the buckle more efficiently and safely.
Choosing your band
A 41 band (3.5 mm width), which I prefer, or thinner bands (e.g., 240 band, 2.5 mm width) can be easily placed with scleral tunnels. Tunneling is the most efficient technique in my hands. Broader bands (e.g., 42 band, 4 mm width) offer wider indentation but are better suited for sutured fixation. When using a 240 band in a combined scleral buckle with vitrectomy, consider placing it farther back from the rectus muscles than you would the 41 because the smaller width provides less posterior coverage.
Tunneling your buckle
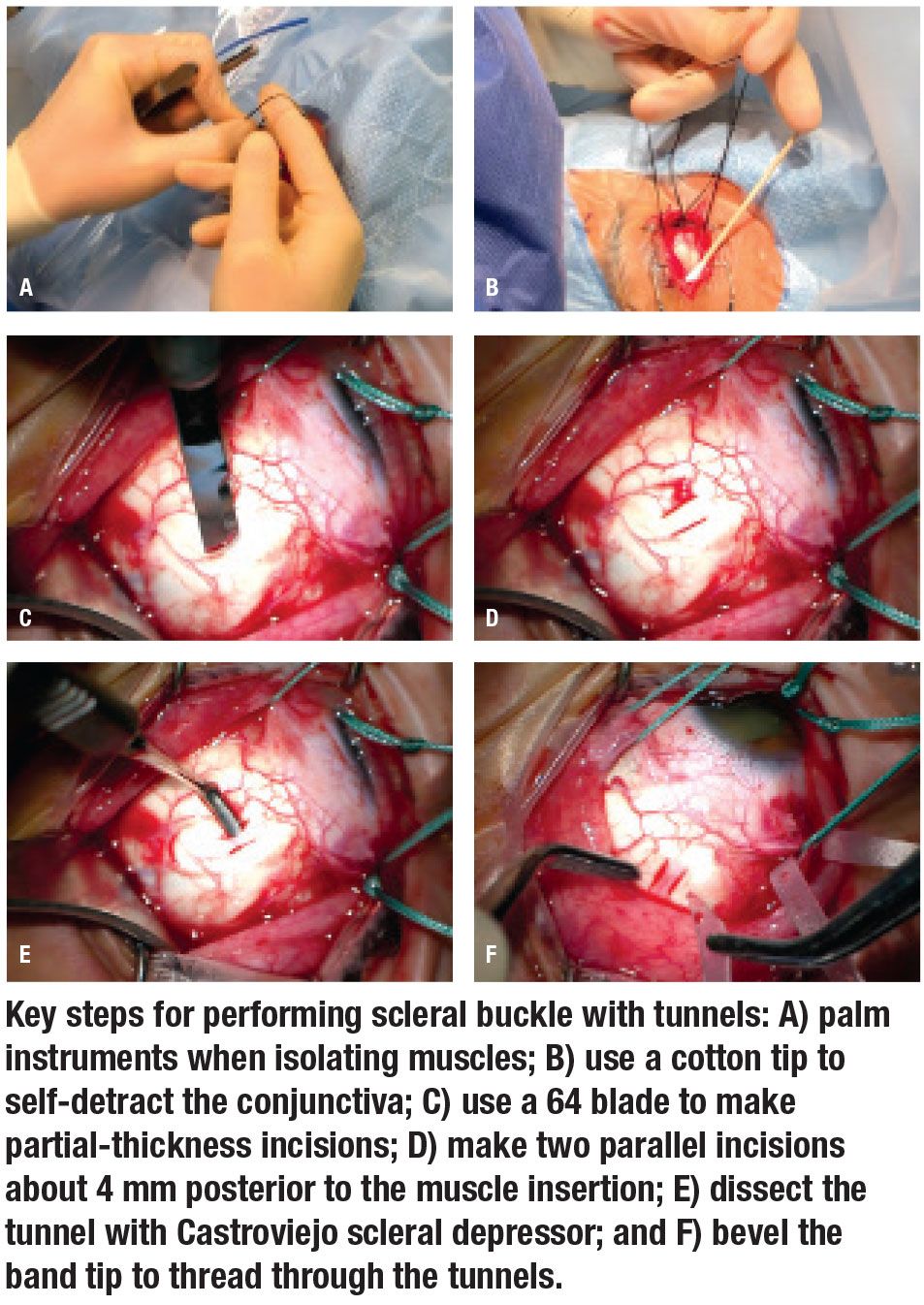 |
Create scleral tunnels by making two parallel, radial, partial thickness incisions with a 64 blade and dissecting the bridging sclera with a Castroviejo scleral dissector. Aim to make the tunnels about 0.5 mm wider than the band width. Trimming the band ends to a point with a bevel helps pass the band without an assistant. To make the tunnel wider, extend posteriorly (and not anteriorly) because the band will slide toward the anterior-most edge of the tunnel. If you’re new to buckling, aim to cause 1 mm of indentation, which can be done by tightening the circumference of a flush buckle by 6.28 mm (C=2π r).1
Perforation
During the initial sclera incisions, the appearance of uveal tissue, vitreous or subretinal fluid indicates scleral perforation. Ease tension on the muscle sutures to avoid further extrusion. Fortunately, the scleral perforation will be supported on the buckle, but close the perforation using a 7-0 vicryl suture. You can still tunnel that quadrant, but restart away from the perforation.
Check the sclera
In eyes with thinner sclera, I’ll suture the band in lieu of scleral tunnels (5-0 nylon on a spatulated needle). In patients with severe ectasia, you may not be able to tunnel or suture a buckle safely. If only one quadrant is involved, then you can skip this quadrant altogether. For more than one quadrant, than I would defer placement of an encircling band.
Elements
A tire can be used to selectively increase indentation. When adding a tire for a 240 band, I use a 287; for a 41 band, use a 287WG (wide groove). You can tunnel the other quadrants of the buckle, but suture in the quadrant(s) of the tire, placing the suture at least 1 to 2 mm anterior and posterior to the tire. The farther the sutures are from the tire, the greater the indentation. To support more posterior pathology, use meridional elements such as the 103, 106 or 112 implant (3, 6 and 12 mm in circumferential width, respectively). Meridional elements slide under the buckle and don’t need to be sutured.
Corticosteroids
In younger patients or if there’s extensive cryotherapy, I use sub-Tenon’s triamcinolone (Kenalog) and a short course of postoperative low-dose oral corticosteroids. RS
REFERENCE
1. Skondra D, Westerfeld C, Vavvas DG, Modified controlled encircling scleral buckle for retinal detachment. J Vitreoretin Dis. 2017;1: 314–316.



