
 |
Bios Dr. Suzue is a clinical instructor at Osaka University, Japan. |
Fovea-sparing internal limiting membrane peeling is a surgical technique used to treat myopic traction maculopathy (MTM) in highly myopic eyes (Figure 1). This technique involves ILM peeling around the fovea while intentionally leaving a small area of intact ILM over the fovea.
Standard, or complete, ILM peeling for MTM carries a risk of postoperative macular hole formation in about 10 percent of patients. Therefore, fovea-sparing ILM peeling is an effective strategy for preventing MH and subsequent visual impairment (Figure 2). Here, we present pearls for performing successful fovea-sparing ILM peeling.
Surgical techniques
• Selecting the right forceps. These eyes have a long axial length, so ILM peeling is challenging to perform using standard ILM forceps. Creating sclerotomies 4.5 to 5 mm from the limbus helps in reaching the macula. If you need additional reach to the macula, such as in patients with an axial length >30 mm, long-shaft ILM forceps are an option.
• Residual vitreous cortex removal. We routinely use triamcinolone to identify the status of the posterior vitreous detachment and the presence of residual vitreous cortex. If no PVD exists, gentle induction of the PVD is in order because the posterior hyaloid often attaches to the macula.
Even if a PVD does exist, the vitreous cortex is typically present due to vitreoschisis, often leaving remnants adhering to the macula and blood vessels.
Repeated staining with triamcinolone and the use of forceps, a Tano scraper and a Finesse Flex loop can facilitate the efficient removal of the vitreous cortex.
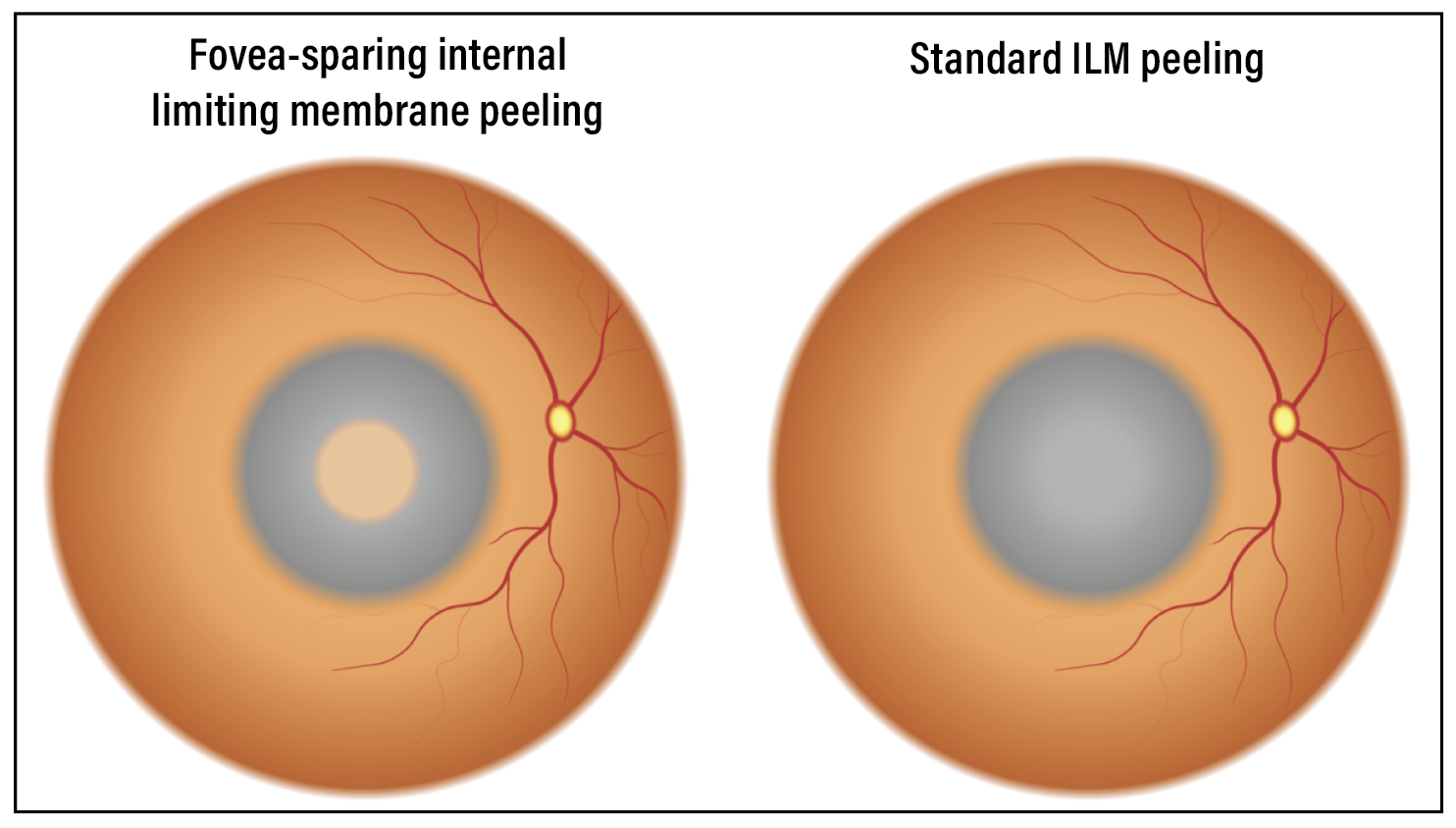 |
| Figure 1. Schematic of fovea-sparing internal limiting membrane peeling and standard, or complete, ILM peeling. |
• Staining of the internal limiting membrane. After removing the residual vitreous cortex, the ILM is well stained with indocyanine green or Brilliant Blue G. Gentle instillation and removal of these dyes are necessary because the fovea is very thin.
The infusion cannula should be oriented toward the mid-periphery or periphery to keep the flow away from the fovea.
• Sparing the fovea. We use forceps to carefully peel off the ILM in a circular fashion around the fovea. Sometimes, the direction of peeling may unintentionally orient toward the fovea, so controlling the direction of peeling is crucial to ensure that it continues in a fovea-sparing manner.
The size of the remaining ILM at the fovea should be approximately 1 disc diameter to prevent postoperative epiretinal membrane. To achieve this, we gently elevate the edge of the remaining ILM, shaping it to be 1 disc diameter at the fovea. We then either leave the edge of the ILM or trim it, depending on the size of the ILM, using scissors or a cutter. When trimming with a cutter, it’s important to ensure that its port is directed away from the fovea.
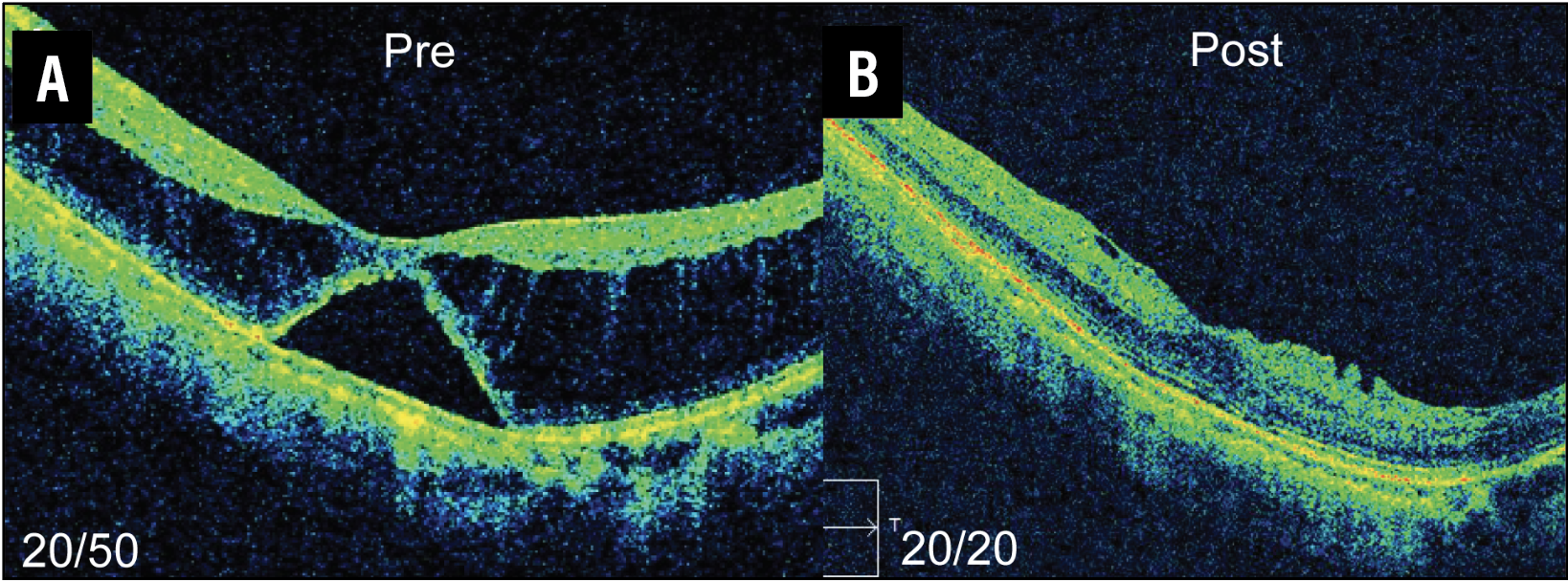 |
| Figure 2. A) Myopic traction maculopathy with foveal retinal detachment. B) Postoperative optical coherence tomography after fovea-sparing internal limiting membrane peeling shows resolution of schisis. |
Applications
Postoperative MH may occur in any type of MTM, including retinoschisis, lamellar MH and foveal retinal detachment. Thus, fovea-sparing ILM peeling is recommended for any type of MTM to prevent postoperative MH.
However, eyes with chorioretinal atrophy are especially prone to MH after standard ILM peeling, likely due to their vulnerable thin retina. Therefore, myopic patients with chorioretinal atrophy may most likely benefit from fovea-sparing ILM peeling. RS
REFERENCES
1. Shimada N, Sugamoto Y, Ogawa M, Takase H, Ohno-Matsui K. Fovea-sparing internal limiting membrane peeling for myopic traction maculopathy. Am J Ophthalmol. 2012;154:693-701.
2. Ho TC, Chen MS, Huang JS, Shih YF, Ho H, Huang YH. Foveola nonpeeling technique in internal limiting membrane peeling of myopic foveoschisis surgery. Retina. 2012;32:631-4.
3. Shiraki N, Wakabayashi T, Ikuno Y, Matsumura N, Sato S, Sakaguchi H, Nishida K. Fovea-sparing versus standard internal limiting membrane peeling for myopic traction maculopathy: A study of 102 consecutive cases. Ophthalmol Retina. 2020;4:1170-1180.



