
 |
| Bios Dr. Wang is a vitreoretinal surgery fellow at Mass Eye and Ear and Harvard Medical School, Boston. Dr. Kim is an assistant professor of ophthalmology at Mass Eye and Ear/Schepens Eye Research Institute and Harvard Medical School. Dr. Hahn is a partner at New Jersey Retina in Teaneck. DISCLOSURES: Dr. Hahn disclosed serving as a consultant to DORC. |
Vitreoretinal surgeons are often tasked with peeling visually significant epiretinal membranes off of the macula. Particularly adherent ERM can be difficult to remove entirely, posing a greater risk of iatrogenic trauma and/or postoperative recurrence. Here, we discuss some tips and tricks that can help ensure a complete and successful ERM peel.
Initiating the peel
Identifying the proper spot to initiate the peel can be half the battle. Preoperative optical coherence tomography can help identify areas to avoid (e.g., areas of macular or nerve fiber layer schisis) and areas to target (e.g., raised areas of membrane that are situated away from the fovea). The ideal initiation spot should also allow for maximum dexterity and control of your chosen instruments with minimal reaching.
Initiation of the flap can be accomplished by aligning the internal limiting membrane forceps over the edge or ridge of the ERM and gently pinching, lifting and releasing. Alternatively, a membrane scraper or the Finesse loop (Alcon) can be used to gently initiate a flap, most effectively over a blood vessel at the edge of the macula. In our experience, the Finesse loop has a slightly longer reach than standard ILM forceps and can prove useful in high myopes.
Triamcinolone vs. BBG (or ICG)
When you encounter difficulty in initiating the flap, you can apply membrane stains to improve your visualization. Triamcinolone, while not exactly a stain, can be used to highlight the surface of the membrane and any elevated ridges as the microparticles settle and adhere to the surface of the membrane.
True stains such as indocyanine green or Brilliant Blue G (BBG, Tissue Blue, DORC) effectively stain the ILM underlying the ERM, making membrane flaps and edges at the interface of “negative staining” obvious to the surgeon.
 |
|
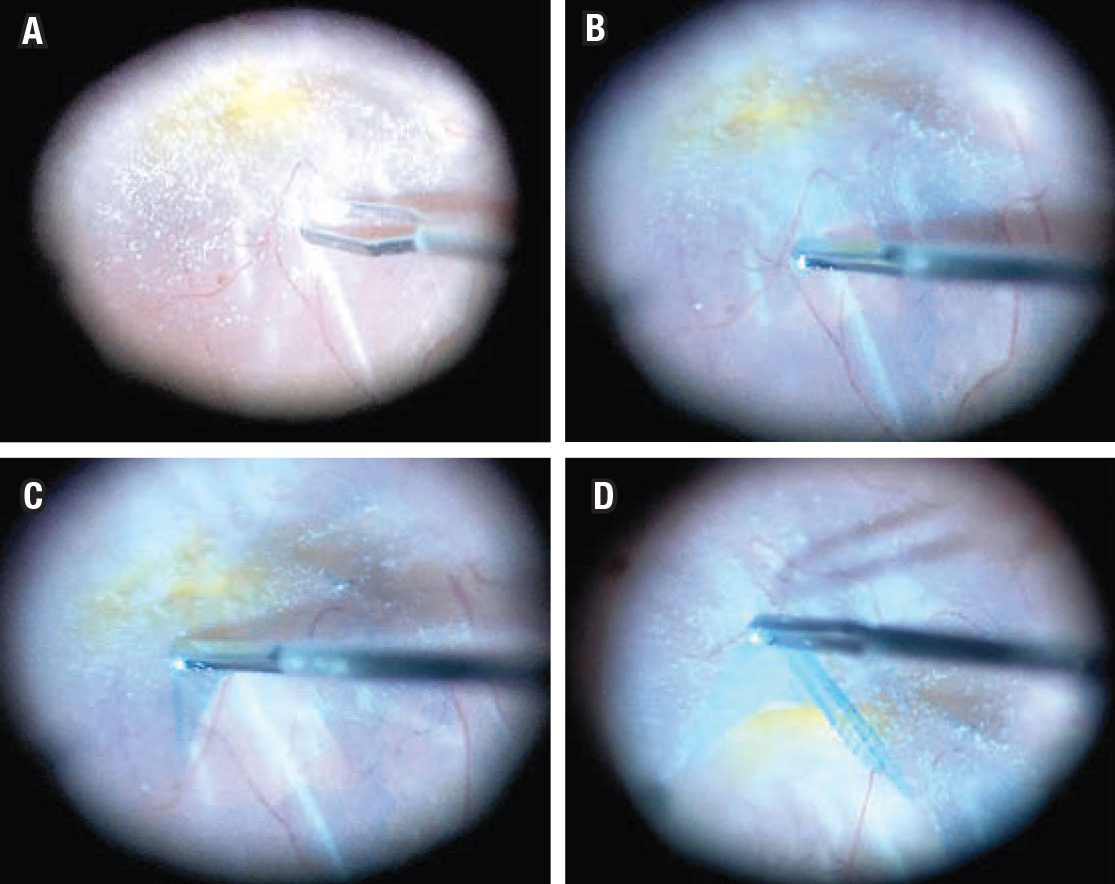
Four steps for performing an easier epiretinal membrane peeling. A) Initiate the peel at the ERM edge with the internal limiting membrane forceps after triamcinolone administration. B) Following Brilliant Blue G staining, align the forceps parallel to and over the edge of membrane, avoiding a deep pinch. C) Pull the initiated flap tangentially along the retinal surface. D) Extend the flap edge circumferentially. |
We prefer BBG and achieve a very effective stain by injecting under direct visualization with a soft-tip cannula aimed over the macula but away from the fovea. We hold the light pipe and the injection cannula in place for one minute to avoid inadvertent dye washout, as the dye settles over the macular area because of its high specific gravity. We then proceed with aspiration of the dye using the vitrector.
Keep forceps tangential to the surface
Once you’ve initiated and visualized a clear flap, you can use the ILM forceps to tangentially peel the membrane in a circumferential manner off the macula and fovea. The applied force should be steady and even. If the patient is a high myope, you may need longer instruments to keep the forceps tangential to the surface and to preserve maximum dexterity of the instruments.
Consider taking the ILM
When confronted with a particularly adherent ERM, we may opt to also peel the underlying ILM. Restaining after ERM peeling can ensure that residual ILM is appropriately visualized and removed. Often, ILM may already have been removed if the adhesive force between an adherent ERM and ILM exceeds that between the ILM and the underlying retina.
Bottom Line
Keep in mind throughout the procedure the goal of ERM peeling: Remove visually significant membrane as efficiently as possible without damaging the macula. Proper visualization and positioning are key to achieving a successful peel. RS



