
Non-aphakic Patients
In most non-aphakic patients, oil overfill is rare, as it immediately results in
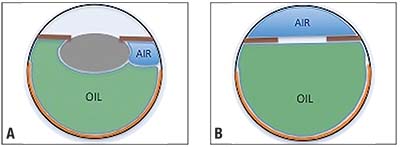 |
| Figure. Air sequestered within the eye will lead to an underfill of silicone oil. A wide-angle viewing system can visualize sequestered air (A), which should be removed. In aphakic patients (B), filling the anterior chamber with air allows easy estimation of the posterior chamber volume for silicone oil filling. These tips apply for an air-oil exchange. Apply alternative techniques when performing a direct fluid-oil exchange. |
Underfill results as the air is quickly absorbed and fluid replaces it. To avoid this, I recommend always inserting the light pipe back in the eye following completion of silicone oil filling to look for sequestered peripheral air bubbles. Aspirating these bubbles with an extrusion cannula (it helps to pull out the silicone tip) or the vitreous cutter followed by additional oil placement as needed to achieve a normal pressure will guarantee a perfect oil fill.
Aphakic Patients
For aphakic patients, oil fill can be more complicated. Caution is needed to prevent both overfill (oil migrating into the anterior chamber) and underfill. I recommend adding an air bubble to fill both the anterior and posterior chambers. I then fill the posterior chamber with oil until I see the oil-air interface just posterior to the iris plane and top off to a normal pressure by palpation.
As above, I then insert a light pipe to remove any posteriorly sequestered air. By the first postoperative day, the air in the anterior chamber will be replaced by fluid, and the fill should be perfect. Of course, an inferior iridectomy is important.
If oil is inadvertently overfilled, the oil-air interface will migrate into the anterior chamber and overfill is easy to identify. Extruding this excess oil and simultaneously infusing air, which will rise through the oil to refill the anterior chamber, will similarly ensure a perfect fill. With an air-filled anterior chamber in aphakic individuals, overfill is also rare unless an incision in the anterior chamber allows air to escape. This is because the oil does not rise above the air, and overfill would lead to an immediately firm eye.
These techniques work well in my hands and require no additional instrumentation or cost. Others have reported similar approaches using an extrusion cannula to completely remove air under direct visualization during oil infusion or viscoelastics to fill the anterior chamber.
Regardless of the technique, understanding the mechanisms of silicone oil underfill and overfill is critical to ensuring the optimal fill every time using the technique that works best for you.
Dr. Hahn is an associate at NJRetina in Teaneck, N.J.



