
 |
 |
Despite the advent of microincision vitrectomy surgery, up to 38 percent of sclerotomy sites are sutured to achieve proper wound closure after 23- and 25-ga. pars plana vitrectomy.1-7 Risk factors for a leaking sclerotomy include high myopia, thin sclera, multiple instrument exchanges, retinal detachment repair, prior history of PPV, extended peripheral vitrectomy and combined phacovitrectomy.1,2
Most surgeons opt to suture leaking sclerotomy sites to minimize the risks of postoperative hypotony and endophthalmitis. Others may suture nonleaking sclerotomies to mitigate the chance of postoperative leaks from blinking or eye rubbing to ensure a complete fill with the tamponade agent of choice (air, gas or oil). Nevertheless, disadvantages of suturing wounds include increased operating time, postoperative patient discomfort, episcleritis, pyogenic granuloma formation and surgically induced astigmatism.
Several alternative techniques to suturing sclerotomy wounds have been described, including scleral wound hydration, adhesive glue, conjunctival cautery or the use of a lightbulb/fine needle to guide removal of the cannula and apply scleral pressure.1,8
All of these techniques have associated limitations. Identifying the edges of the sclerotomy wound for hydration is not always possible when conjunctival chemosis or subconjunctival hemorrhage is present. Glue is time-consuming and can be very uncomfortable for the patient postoperatively. Cautery has been associated with scarring and inflammation with variable efficacy.
Scleral needling technique
 |
We describe a novel scleral needling (SN), or “scleral acupuncture”, technique to achieve sutureless closure of leaking sclerotomy sites following 23- or 25-ga. PPV.1
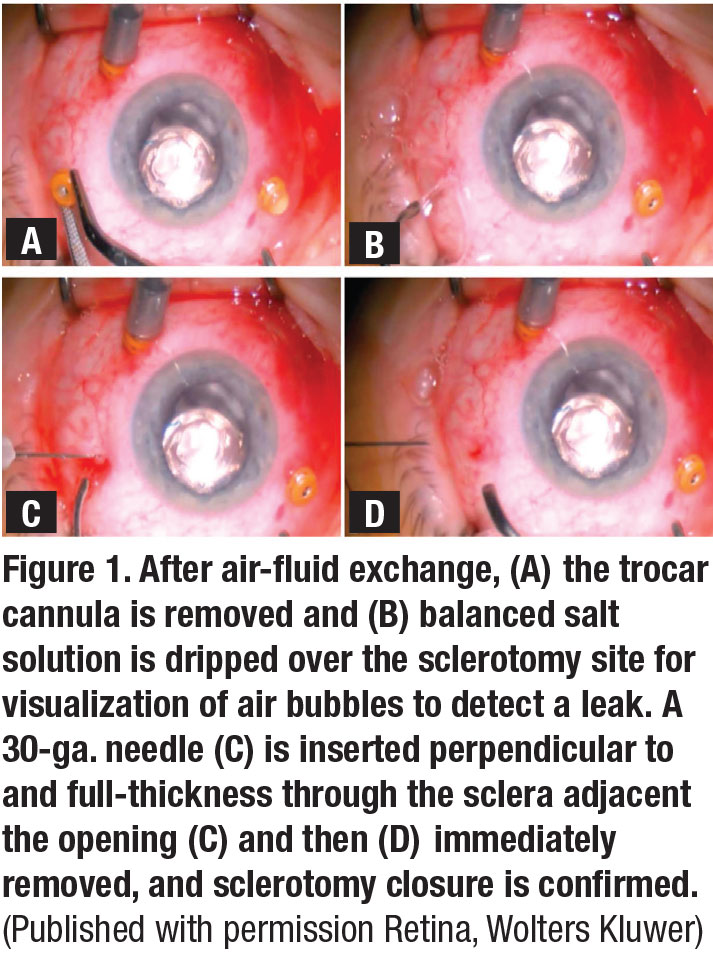
In this technique, following the removal of the trocar cannula, a 30-ga. needle attached to a closed 1-mL syringe is inserted perpendicularly within the sclerotomy wound bed and quickly removed. Subsequently, a 19-ga. cannula is used to apply gentle pressure over the sclerotomy site for three seconds (Figure 1). Any residual leakage is then detected with basic salt solution irrigation and the needling is repeated if necessary (Video).
We performed a retrospective comparison of 203 eyes undergoing PPV including 105 eyes prior to the introduction of scleral needling (pre-SN group) and 98 eyes following the integration of scleral needling in our practice (post-SN). Our results suggested that 39 percent of eyes in the pre-SN group required suturing vs. only 2 percent of eyes in the post-SN group.
Most importantly, we found no significant difference in rates of hypotony or intraocular pressure between either cohort on days 1 to 20 postoperatively. In fact, SN was associated with a significantly higher incidence of subconjunctival hemorrhage and better visual acuity postoperatively compared to eyes in the pre-SN cohort.
How does scleral needling work?
 |
Although the exact mechanism of wound closure with this technique isn’t clear, two mechanisms have been proposed. Some speculate that SN draws vitreous to the inner os of the sclerotomy wound, plugging it. We’ve demonstrated this using vitrectomized cadaveric eyes with an endoscope illumination system.
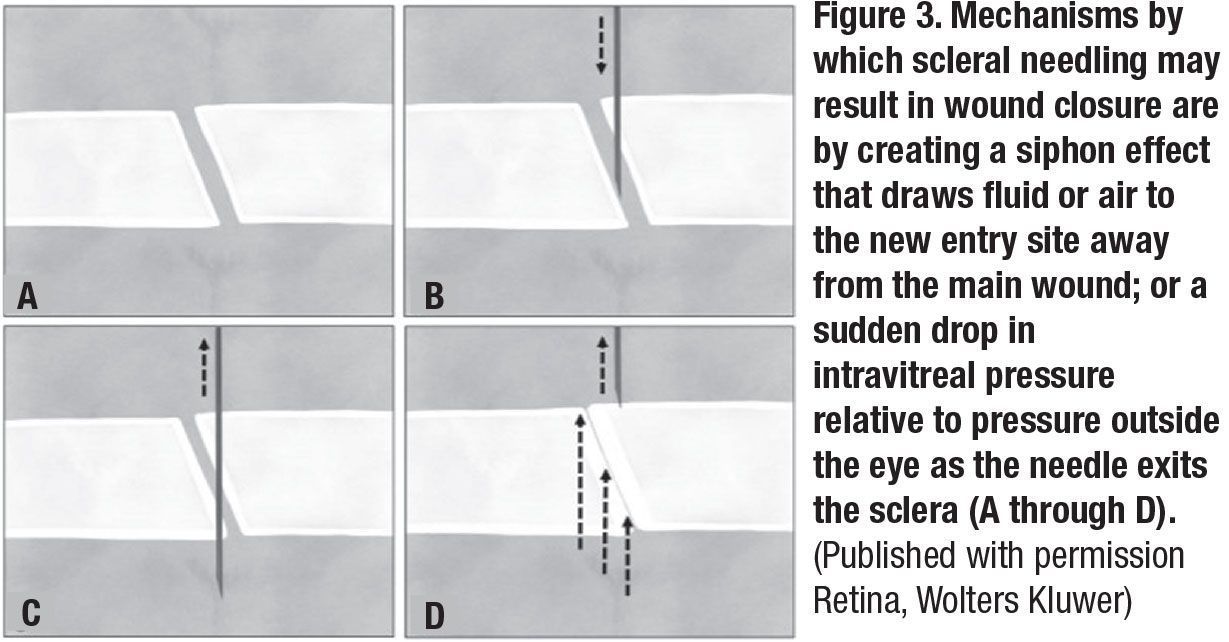
Using intravitreal triamcinolone, we observed that needling draws vitreous strands to the needle-entry site (Figure 2). Secondly, scleral needling may create a siphoning effect that draws fluid or air to the new entry site away from the main wound, resulting in wound closure.1 Another possibility is that a sudden drop in intravitreal pressure relative to the pressure outside the eye created by the exiting needle from the sclera may close the wound (Figure 3).9-11
Technical pearls
At the end of the case, we often do at least a partial fluid-air exchange to help identify and air leaking from the corneal wounds at the end of the case. We prefer to use a 30- or 27-ga. needle, both of which work effectively. Our usual routine is to partially remove the trocar and then pre-place a 30-ga. needle attached to an empty TB-syringe perpendicular to the sclera just adjacent to the trocar in the bed of the scleral wound. As we remove the trocar, the needle is dipped into the vitreous cavity, about halfway down the needle tip and then removed entirely.
 |
A blunt 19-ga. cannula, usually attached to the irrigating BSS bottle, is then used to firmly press on the scleral wound bed. A few drops of BSS are used to inspect the wound for any air leaks, and if we note any, we needle the sclera again and use cannula to press on the wound.
Some cases can require up to five scleral needles, but about 98 percent of the wounds stop leaking and close completely. This technique works very well in both air-filled and silicone-filled eyes.
Bottom line
Scleral needling is a simple, safe, and effective technique to achieve wound closure following 23- and 25-ga. PPV. RS
 |
‘Scleral Acupuncture,’ i.e., needling for sutureless closure from Retina Specialist on Vimeo.
References
1. Felfeli T, Altomare F, Mandelcorn ED. Sutureless closure of 23- and 25-gauge leaking sclerotomies with the scleral needling technique. Retina. 2020;40:838-844.
2. Woo SJ, Park KH, Hwang JM, et al.Risk factors associated with sclerotomy leakage and postoperative hypotony after 23-gauge transconjunctival sutureless vitrectomy. Retina 2009;29:456–463.
3. Chieh JJ, Rogers AH, Wiegand TW, et al. Short-term safety of 23-gauge vitrectomy surgery. Retina 2009;29:1486–1490.
4. Gupta OP, Ho AC, Kaiser PK, et al. Short-term outcomes of 23-gauge pars plana vitrectomy. Am J Ophthalmol 2008;146: 193–197.
5. Duval R, Hui JM, Rezaei KA. Rate of sclerotomy suturing in 23-gauge primary vitrectomy. Retina 2014;34:679–683.
6. Parolini B, Prigione G, Romanelli F, et al. Postoperative complications and intraocular pressure in 943 consecutive cases of 23-gauge transconjunctival pars plana vitrectomy with 1-year follow-up. Retina 2010;30:107–111.
7. Taleb EA, Nagpal MP, Mehrotra NS, et al. Comparison of clinical outcome between 23-G and 25-G vitrectomy in diabetic patients. Oman J Ophthalmol. 2017;10:213-219.
8. Boscia F, Besozzi, G, Recchimurzo N, et al. Cauterization for the prevention of leaking sclerotomies after 23-gauge transconjunctival pars plana vitrectomy: an easy way to obtain sclerotomy closure. Retina. 2011;31:988-990.
9 Panda A, Kumar S, Kumar A, Bansal R, Bhartiya S. Fibrin glue in ophthalmology. Indian J Ophthalmol. 2009;57:371-379.
10. Felfeli T, Mandelcorn MS, Altomare F, Mandelcorn ED. Reply: Sutureless closure of 23-gauge and 25-gauge leaking sclerotomies with the scleral needling technique. Retina. Published online December 30, 2019.
11. Mandelcorn ED, Felfeli T, Mandelcorn MS. Scleral needling technique. Can J Ophthalmol. Published online June 23, 2020.



