
 |
| Bios Dr. Todorich is with Lehigh Eye Specialists, Allentown, Pennsylvania. Dr. Hahn is a partner at New Jersey Retina in Teaneck. DISCLOSURES: Dr. Todorich disclosed relationships with Vortex Surgical, Genentech, Regeneron Pharmaceuticals and Allergan/AbbVie. Dr. Hahn disclosed serving as a consultant to DORC. |
Advances in vitrectomy platforms have automated most parts of vitrectomy surgery so that surgeons can perform critical steps, such as fluid-air exchange, silicone-oil injection or laser retinopexy efficiently and independently.
Yet, for peripheral vitrectomy, particularly in primary retinal detachment repair, many of us still use assistants to do scleral indentation. For surgeons in private practice or non-academic institutions, this can be particularly challenging, because assistants aren’t always available. In those cases, retina surgeons may forgo depressed vitreous base shaving or resort to chandelier illumination, which is more expensive.
A low-cost depressor cap
A low-cost, disposable depressor cap (Figure A) compatible with Alcon and Bausch + Lomb light pipes is available from Vortex Surgical. An analogous depressor is available for the DORC Eva system.
The light pipe is inserted in the depressor, which is molded in the shape of a traditional ball-point depressor (Figure B), thus emitting light through the tip that allows for simultaneous depression, transillumination and peripheral vitrectomy (Figures C, D).
For optimal illumination, the light pipe setting is set to maximum on the vitrectomy machine. The tip is made of polished polycarbonate, which maximizes light transmission and allows it to slide into the conjunctival fornix and glide along the scleral surface.
The shaft of the depressor is fortified with a metal hypodermic needle that enhances stiffness and prevents glare from light backscatter. The device accommodates 23-, 25- and 27-gauge instruments.
Ideal cases for the depressor
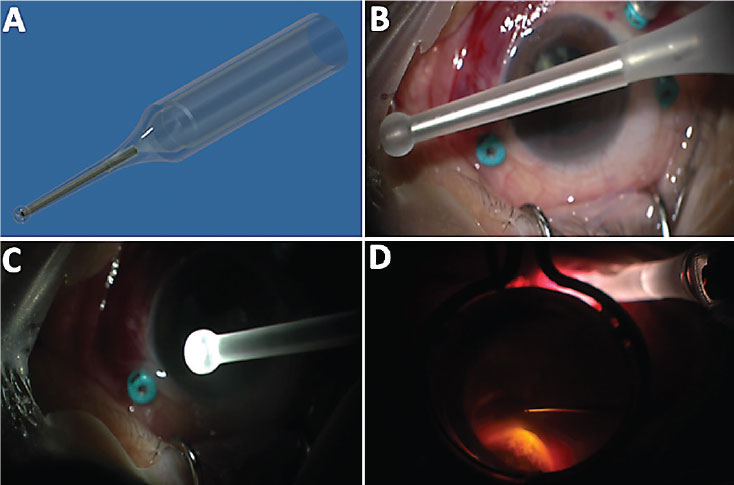 |
| The depressor cap (A) converts any 23- to 27-gauge light pipe into a scleral depressor- transilluminator. The light pipe is inserted with the tip fully seated within the ballpoint end (B) and with the light on (C). Intraoperative view (D) of “task-specific” illumination for simultaneous vitreous base shaving. |
The depressor performs best with lightly pigmented and/or myopic eyes with thin sclera, which permit the most light penetration. In these eyes, effective depression-
transillumination can be visualized on any conventional microscope.
In more pigmented eyes or cases with vitreous hemorrhage, a digital microscope, such as the Alcon
Ngenuity 3D system that can amplify low-level luminance, can enhance dimmer and more challenging viewing. The vitreous isn’t as well visualized as with conventional endoillumination, so you should methodically shave clock hour by clock hour to avoid skip areas, and use adjuvants such as triamcinolone if you need it to enhance the Tyndall effect of the peripheral vitreous.
If you’re using a digital microscope, you can further improve the view of the vitreous by manipulating the light and color settings. The learning curve consists of about a dozen or so cases to get used to “task specific” rather than diffuse conventional endoillumination, as the video demonstrates, and to train your hands to follow each other in both pseudophakic and phakic eyes.
This low-cost device converts any light pipe into a depressor-transilluminator, which gives you complete and independent control of peripheral vitrectomy. RS



