Take-home points
|
 |
|
Bios Dr. Walter is a partner with Retina Consultants PC in Hartford, Connecticut, vice chief of the ophthalmology service at Hartford HealthCare and clinical assistant professor at the University of Connecticut School of Medicine, Farmington. Dr. Archambault is a second-year resident at New England Eye Center, Tufts Medical Center, Boston. DISCLOSURES: Dr. Walter disclosed relationships with Allergan/AbbVie, Bausch + Lomb, Castle Biosciences, EyePoint Pharmaceuticals, Genentech/Roche, Novartis, Regeneron Pharmaceuticals, Apellis Pharmaceuticals and Spark Therapeutics. Dr. Archambault has no relevant relationships to disclose. |
More than 20 percent of the U.S. population will develop epiretinal membranes by the sixth and seventh decades of life.1 A complete or partial posterior vitreous detachment typically precedes membrane formation, leaving hyaloid remnants and activated hyalocytes on the macular surface which serve as the scaffold for membrane formation.2
Pars plana vitrectomy with internal limiting membrane peeling has become the gold standard procedure for treatment of full-thickness macular holes (FTMH) and epiretinal membranes (ERM).3,4 ILM peeling has been shown to improve success rates for FTMH closure5 and reduce postoperative ERM recurrence.6
The existing gold standard for ILM peel involves the use of ILM forceps, but a number of techniques have emerged that forgo the use of forceps. This article will explore alternative approaches for performing ILM peel for FTMH and ERM.
The ILM is a type IV collagen membrane on the macular surface, produced by the footplates of Müller glia, that thickens over time. These age-related changes at the vitreoretinal interface are believed to contribute to the pathogenesis of vitreoretinal interface disorders such as FTMH and ERM.7,4
Standard ILM peeling with forceps
The standard procedure involves performing a three-port pars plana vitrectomy to remove the vitreous body and, if necessary, surgically inducing a posterior vitreous detachment to remove cortical vitreous from the macular surface. Chromovitrectomy is performed with a vital dye, such as indocyanine green or Brilliant Blue, to stain the ILM.
The ILM is peeled to remove ERMs and other tractional forces acting on the macular surface. Classically, the surgeon creates the ILM rhexis using either ILM forceps (“pinch and peel”) or a second instrument, such as a Finesse Flex Loop (Alcon) or Tano Diamond Dusted membrane scraper (Bausch + Lomb). The surgeon then completes the ILM peel using forceps to manually peel and remove ILM fragments from the eye.8
 |
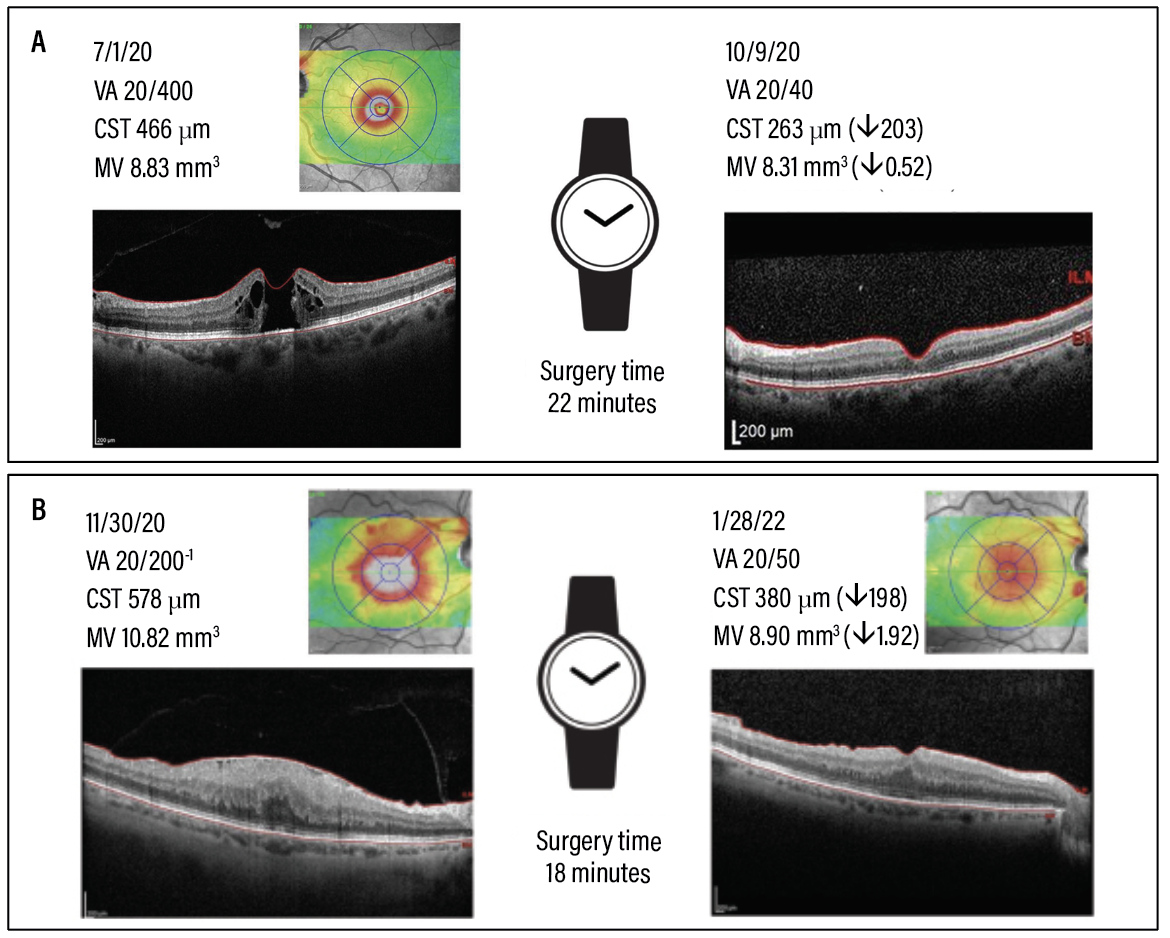
| Figure 1. Examples of internal limiting membrane peeling approaches used in patients in our consecutive case series of cutter-based membrane peeling. A) The first patient with successful closure of a large full-thickness macular hole. B) Successful removal of an epiretinal membrane in the last patient in the series. Both patients had clinically significant improvements in visual acuity, macular volume and central subfield thickness at one month postoperatively vs. baseline. |
Alternative approaches to ILM peeling
 |
Several vitreoretinal surgeons have previously described techniques for ILM peeling without the use of forceps. Both Tim Murray, MD, MBA, and Goran Petrovski, MD, PhD, have independently reported cases of ILM peeling using only the vacuum aspiration function of the vitrectomy probe.9 Recently, Carl Awh, MD, developed a new instrument (Awh MVP Micro Vacuum Pick, Katalyst Surgical) specifically designed for ILM peeling by vacuum aspiration.10 In all these reports, the patients had anatomical and functional improvements without iatrogenic retinal damage.
Evolution of my technique
The Finesse Flex Loop has always been my preferred instrument for creating the ILM rhexis. After initiating the ILM rhexis, I used to switch to an ILM forceps to peel and remove the ILM fragments.
However, like my colleagues,9-10 I recently discovered that ILM peeling can be performed with ease and efficiency using the vacuum aspiration function of the vitrectomy handpiece. This technique has several apparent advantages. Most importantly, they include the ability to peel and remove ILM tissue without removing instruments from the eye.
As cutter-based membrane peeling became my preferred technique, Dr. Archambault and I wanted to examine the practicality, safety and efficacy of cutter-based membrane peeling compared with conventional forceps-based peeling. We hypothesized that this technique could minimize the number of instrument exchanges, potentially reducing surgical time and the risk of intraoperative complications.
We conducted a retrospective chart review to compare patient outcomes between the different peeling techniques for patients undergoing vitrectomy with ILM peeling. We first presented our results last year at the 50th annual meeting of the American Society of Retina Specialists in New York City.11
Surgery time reduced 10 minutes
Between April 2020 and December 2021, I performed 92 consecutive vitrectomies with ILM peeling for FTMHs (n=30, 32 percent) and ERMs (n=62, 68 percent) at a single ASC in Connecticut. Baseline demographics, visual acuities, macular volumes (MV) and central subfield thicknesses were similar between the two groups. We followed the patients for a minimum of three months postoperatively (Figure 1, page 33).
For all the operations, I used a 25-gauge vitrectomy platform (Constellation Vision System; Alcon) and “heavy” ICG for ILM staining. I initiated the ILM rhexis using a Finesse Flex Loop. The only modifications to the procedure were whether the ILM peeling was done using the ILM forceps (n=12) or a 25-gauge vitrectomy probe (“cutter”) (n=80).
Total surgical time was the primary outcome of our study. We found that cutter-based membrane peeling significantly reduced the total operative time by an average of 10 minutes (p=0.001).
Safety and efficacy outcomes
Knowing that cutter-based membrane peeling could significantly reduce surgical time, we sought to establish the safety and efficacy of this technique.
Patients in both groups had significant improvements in visual acuity (p=0.001), macular volume (p=0.001) and CST (p=0.001) three months postoperatively compared to preoperative values. In addition, the cutter-based technique resulted in high rates of single-operation anatomic success (>96 percent).
We reported no intraoperative complications, such as iatrogenic macular holes, retinal breaks, retinal detachments or choroidal detachments, in either group. There was only one case of postoperative RD in the cutter-based group after three months, which is less than the expected 2-to-3-percent cumulative incidence of RD observed in large claims-based studies of vitrectomy with ILM peeling.12
 |
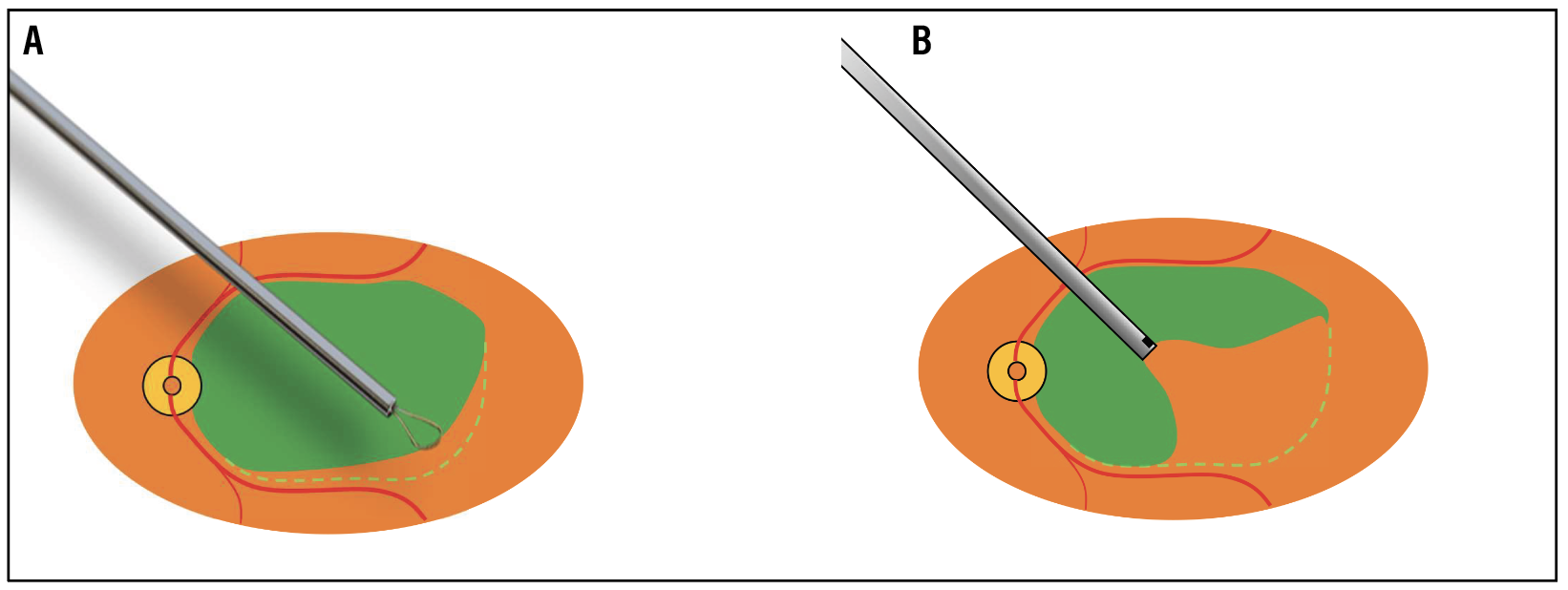
| Figure 2. A two-step technique for internal limiting membrane peeling without forceps. A) We use a flexible loop scraper to create a 180-degree rhexis of the ILM along the arcades. B) The ILM flap is then peeled using the vitrectomy probe on aspiration mode to release all traction on the fovea. Once the ILM rhexis is completed, the amputated ILM flap is aspirated into the port. Key: VA = visual acuity; CST = central subfield thickness; MV = macular volume. |
Tips and tricks for cutter-based peeling
 |
You may feel somewhat clumsy when starting with the cutter-based technique. Peeling and manipulating the ILM with the cutter will require new coordination and movements. However, in my experience the learning curve was very short because we already perform many of the required maneuvers during other vitreoretinal surgeries. Here are key steps in the procedure.
= Initiating the peel. I typically initiate the peel using a Finesse Flex Loop to create a 90-to-180-degree curvilinear ILM rhexis along the inferotemporal arcade (Figure 2A). To engage the ILM flap with the vitrectomy handpiece, turn the cutter off. Position the cutter directly in front of or behind the rhexis edge with the port aimed towards the middle of the flap.
= Increasing the vacuum. Next, use proportional foot pedal control to increase the vacuum until the ILM tissue occludes the port. Once the port is occluded, the vitrectomy handpiece will function like closed forceps as long as a moderate level of vacuum aspiration is maintained (Figure 2B).
= Peeling maneuvers. Peeling can be done using a variety of simple maneuvers, including lateral movements of the cutter, vertical movement of the cutter, rotation of the cutter port and/or adjusting the amount of vacuum aspiration.
= Coordinating cutter maneuvers. Exercise caution when coordinating cutter maneuvers with increasing proportional vacuum because you can easily tear the flap if the suction is too great.
= Releasing traction. Take care when releasing traction on the fovea. With low aspiration, carefully rotate the cutter port or gently “tug back” with the probe, to tease the ILM off the fovea. Once all traction has been released from the fovea, the remaining 180 degrees of the ILM rhexis can be completed with full aspiration.
 |
This technique has helped me save time and reduce my ASC instrument costs. I was glad to see that my patients have had excellent anatomic and visual outcomes without sacrificing safety. I no longer use ILM forceps except in special circumstances, such as for ILM peeling under perfluorocarbon liquid. Over the past three years, I’ve completed hundreds of cases, using ILM forceps on only four occasions. There’s also no doubt that the decreased operative time contributes to increased patient satisfaction.
Bottom line
Based on our study, we believe that cutter-based membrane peeling is a safe and effective alternative to forceps-based peeling. This technique can reduce operative time and surgical case costs while providing the same high quality of patient care. RS
REFERENCES
1. Ng CH, Cheung N, Wang JJ, et al. Prevalence and risk factors for epiretinal membranes in a multi-ethnic United States population. Ophthalmology. 2011;118:694-699.
2. Stevenson W, Prospero Ponce CM, Agarwal DR, Gelman R, Christoforidis JB. Epiretinal membrane: optical coherence tomography-based diagnosis and classification. Clin Ophthalmol. 2016;10:527-534.
3. Duker JS, Kaiser PK, Binder S, et al. The International Vitreomacular Traction Study Group classification of vitreomacular adhesion, traction, and macular hole. Ophthalmology. 2013;120:2611-2619.
4. Spiteri Cornish K, Lois N, Scott NW, et al. Vitrectomy with internal limiting membrane peeling versus no peeling for idiopathic full-thickness macular hole. Ophthalmology. 2014;121:649-655.
5. Sandali O, El Sanharawi M, Basli E, et al. Epiretinal membrane recurrence: Incidence, characteristics, evolution, and preventive and risk factors. Retina. 2013;33:2032-2038.
6. De Novelli FJ, Goldbaum M, Monteiro MLR, Aggio FB, Nóbrega MJ, Takahashi WY. Recurrence rate and need for reoperation after surgery with or without internal limiting membrane removal for the treatment of the epiretinal membrane. Int J Retina Vitreous. 2017;3:48.
7. Berton M, Robins J, Frigo AC, Wong R. Rate of progression of idiopathic full-thickness macular holes before surgery. Eye. 2020;34:1386-1391.
8. Almony A, Nudleman E, Shah GK, et al. Techniques, rationale, and outcomes of internal limiting membrane peeling. Retina. 2012;32:877-891.
9. Lumi X, Petrovski BE, Petrovski G. Simple new technique for macular pucker peel without forceps. Frontiers in Medicine. 2022;9:947578.
10. Awh CC, Bass EJ. A microsurgical vacuum pick for membrane peeling without forceps during vitreoretinal surgery. Ophthalmic Surg Lasers Imaging Retina. 2020;51:196-199.
11. Walter S. Cutter-based vs. forceps-based membrane peeling for removal of epimacular membranes. American Society of Retina Specialists’ 40th annual scientific meeting. New York, NY; July 14, 2022.
12. Vaziri K, Schwartz SG, Kishor KS, et al. Rates of reoperation and retinal detachment after macular hole surgery. Ophthalmology. 2016;123:26-31.



