
 |
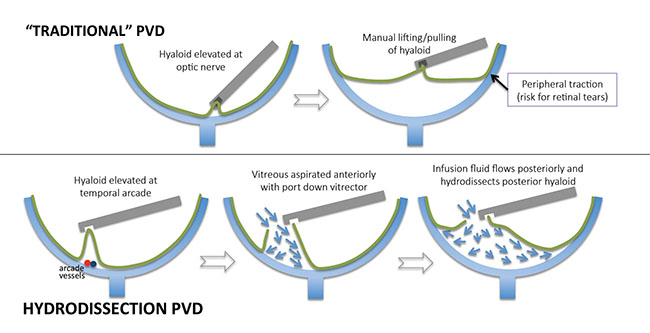
| Figure. Traditional posterior vitreous detachment (top) involves manual elevation of the posterior hyaloid from the optic nerve to the periphery, which can lead to peripheral retinal traction and tears. Hydrodissection PVD begins with aspirating a portion of the posterior hyaloid over a temporal vascular arcade with the port down. Once space is created, vitrectomy is performed 360 degrees circumferentially in the mid-peripheral vitreous with the port down and full vacuum. As vitreous aspirates anteriorly, infusion fluid flows posteriorly, gently hydrodissecting the hyaloid off the retina to the vitreous base. |
In this pearl, Vincent Y. Ho, MD, and Gaurav K. Shah, MD, present “hydrodissection PVD,” their preferred method of surgical induction that they propose minimizes traction at the optic nerve and retina and reduces the risk of iatrogenic retinal tears.
Step by Step
First, apply kenalog to highlight the vitreous, then hold the vitrector near a temporal vascular arcade port-down (facing the retina) with maximum aspiration (no cutting) to engage a portion of the posterior hyaloid. Maintain maximum aspiration until a space appears between the posterior hyaloid and retina.
The next step is to initiate cutting along with maximum aspiration. Use the vitrector with the port still facing downward to create a 360-degree circumferential hyaloidectomy at the level of the midperiphery. In doing so, the vitreous flows anteriorly into the vitrector port while the infusion fluid is forced posteriorly, resulting in hydrodissection of the remaining posterior hyaloid off the retinal surface and out to the vitreous base insertion.
Typically, the last hyaloid remnant is attached to the nerve, and you can remove it by slowly approaching the posterior pole with the vitrector. Once the posterior vitreous detachment is complete, turn the port to face the vitreous base for peripheral shaving if indicated.
Reduction of Risks
Because this approach uses primarily hydrodissection to separate the hyaloid, as opposed to direct traction with the traditional method, Drs. Ho and Shah believe it reduces the risk of iatrogenic retinal tears and optic nerve traction. They use an EVA by DORC (Exeter, N.H.) vitrectomy platform with 92 percent biased-open duty cycle and augmented infusion that create robust and dynamic flow that they feel is critical to the success of this maneuver. This technique works best in vacuum mode (rise time up to 300 milliseconds, maximum vacuum of 680 mmHg), and can successfully be completed with 20-, 23-, 25- and 27-gauge surgery.
 |
| Watch the Video Watch as Vincent Ho, MD, and Gaurav Shah, MD, describe a novel approach to potentially safer post- erior vitreous detachment induction using hydrodissection. Available at: http://bit.ly/2aWlzk7 |
Dr. Hahn is an associate at New Jersey Retina in Teaneck. Drs. Ho and Shah are with The Retina Institute of St. Louis



