
 |
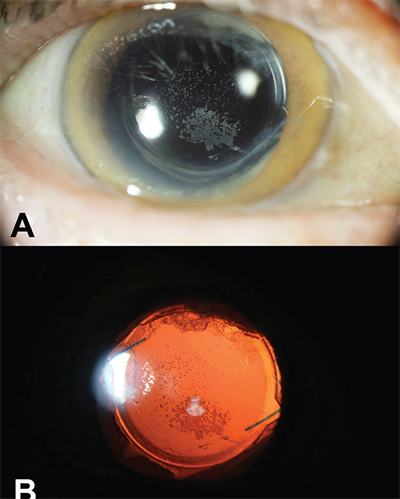
| Figure 1. Slit lamp photography without (A) and with (B) retroillumination shows visually significant posterior intraocular lens deposits with an open posterior capsule. |
Visually significant deposits on the surface of intraocular lenses frequently pose a challenge to retina specialists (Figure 1). Calcific deposits have been noted to develop on the posterior surface of silicone IOLs following YAG capsulotomy in eyes with asteroid hyalosis. Additionally, some hydrophilic acrylic lenses have been found to undergo opacification with deposition of calcium phosphate crystals with time.
Additional cases of visually significant pigment deposition on eyes with pigment dispersion and uveitis as well as deposition of pseudoexfoliative material in the visual axis have been reported. While the cause of IOL opacification is not always clear, intervention is usually needed to augment vision.
A minimally invasive option
The approach to such deposits has ranged from use of an Nd:YAG laser to IOL exchange and sometimes vitrectomy. However, the Nd:YAG laser may be ineffective and can cause IOL pitting. A vitreous cutter may be ineffective in removing the fine granular IOL deposits. Here, Akshay Thomas, MD, MS, of Tennessee Retina describes a minimally invasive technique using an Alcon Finesse flex loop (Figure 2A, B).
Dr. Thomas demonstrates his surgical technique for removing posterior lenticular deposits.
 |
Preoperative evaluation
Key things to note are whether the posterior capsule is intact and where the IOL deposits are located. By the time we are evaluating a patient for IOL deposits, a YAG capsulotomy will often have already been performed.
For this technique, an intact posterior capsule will need to be opened. While it’s most common for the deposits to be on the anterior or posterior surface of the IOL, some deposits may actually be within the substance of the IOL, which would necessitate an IOL exchange.
Surgical technique
This approach to treating lenticular deposits involves the following eight steps:
1. Set up for standard three-port vitrectomy. Position the wrist rest lower than normal as most of the case will require anterior angulation of surgical instruments
2. If the posterior capsule is still in- tact, perform a limited anterior vitrectomy and make a 3-mm central opening with the vitreous cutter.
3. Larger IOL deposits may be amenable to removal with vitreous cutter suction.
4. Insert the flex loop and re- tract the shaft such that the entire loop is exposed.
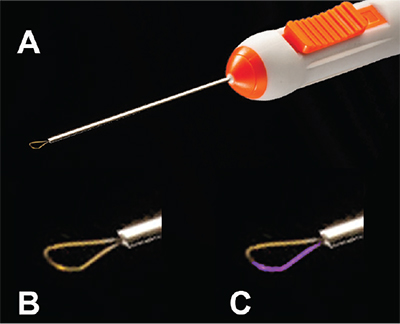 |
| Figure 2. The Alcon Finesse flex loop |
5. Position the loop perpen- dicular to the posterior IOL surface such that only half of the loop is in contact with the lens (Figure 2C).
6. Next, use the loop to gently scrub the back of the IOL to remove the deposits. If the deposits aren’t coming off easily, shorten to loop to in- crease its stiffness and then repeat.
7. Most deposits are usually trapped within the serrations of the loop and may be peri- odically washed off.
8. If a significant amount of deposits are released into the vitreous cavity, a limited vit- rectomy can be performed. You may opt to start off with only one or two ports and place additional ports only if a vitrectomy is required. RS



